Melatonin Shows Real Promise For Chronic Joint, Muscle Pain

(© Tihana - stock.adobe.com)
Melatonin May Do More Than Help With Sleep, Study Suggests In A NutshellFor people who take melatonin before bed, the sleep supplement may be doing something more interesting than helping them drift off. A new analysis of dozens of clinical trials suggests melatonin, the hormone the body produces naturally when the lights go down, may modestly reduce chronic muscle and joint pain. Researchers caution it should be seen as a potential add-on to existing treatments, not a replacement for standard painkillers.
This kind of pain, the aching sort that comes with arthritis, fibromyalgia, or a bad back, is stubborn and hard to treat. Common options like opioids and anti-inflammatory drugs carry real risks, from dependency to stomach damage. So the idea that an inexpensive, widely available supplement could chip away at it is drawing real interest.
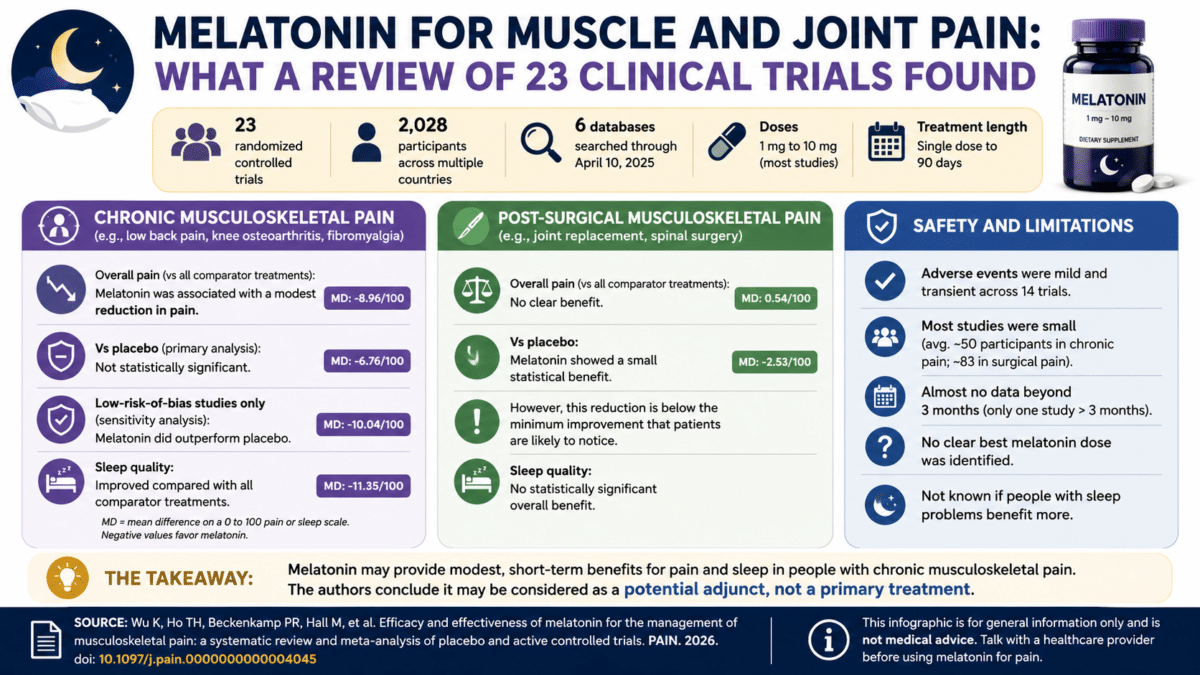
A new review published in the journal PAIN, pooling data from 23 clinical trials and more than 2,000 patients, found that melatonin was tied to less pain and better sleep for people dealing with this kind of pain long-term. The quality of that evidence was rated low to moderate, and researchers were careful to note that similar-looking numbers don’t make melatonin a swap-in for existing pain medications.
Melatonin Eases Chronic Pain, But Not in Every ComparisonTo find out, researchers combed through six major medical databases for every relevant study published through April 2025. They only counted randomized controlled trials, where patients are split into groups at random and nobody knows who got which treatment, since those give the most trustworthy results. Patients had to be dealing with pain lasting three months or longer, or pain from recovering after surgery.
In the end, 23 studies fit the bill, covering more than 2,000 patients from the United States, Iran, Russia, Brazil, Egypt, China, and elsewhere. Almost everyone took melatonin as a pill, in doses from 1 to 10 milligrams, for anywhere from a single presurgery dose to three months of daily use.
For long-term aches like low back pain, fibromyalgia, and arthritis, melatonin edged out other treatments lumped together, and that dip in pain was real, not just noise in the data. Against placebo specifically, the drop wasn’t quite big enough to call proven across the full set of studies. But when researchers zoomed in on only the highest-quality trials, melatonin did pull ahead of placebo in a way that held up.
Recovery pain after surgery told a messier story. Across a dozen trials on patients healing from joint replacements and spinal surgery, melatonin nudged pain down compared with placebo, but only by about two and a half points on a hundred-point scale, too small for most patients to actually notice. Against other painkillers used after surgery, melatonin didn’t pull ahead at all.
 Melatonin eased chronic pain and improved sleep in a new review of over 2,000 patients, though evidence is limited. (Image by StudyFinds)
Better Sleep May Explain Melatonin’s Pain-Relieving Effect
Melatonin eased chronic pain and improved sleep in a new review of over 2,000 patients, though evidence is limited. (Image by StudyFinds)
Better Sleep May Explain Melatonin’s Pain-Relieving Effect
One of the more interesting threads running through this research involves sleep. Pain and bad sleep feed off each other: pain makes it harder to doze off, and a rough night makes pain feel worse the next day. People with long-term pain who took melatonin reported real improvements in sleep quality, and researchers think that might be part of why it eased their pain too, though the review didn’t test that link directly.
That sleep boost didn’t show up in surgery patients. Compared with everything else tried after an operation, melatonin didn’t meaningfully improve how well people slept.
Melatonin’s Effect Size Rivals NSAIDs, But Not the Full StoryPerhaps the most eye-catching comparison in the paper involves NSAIDs, anti-inflammatory pills like ibuprofen that doctors often reach for first with this kind of pain. Melatonin’s relief in chronic cases landed in roughly the same range as what earlier research reports for NSAIDs. That doesn’t mean the two are interchangeable: evidence behind melatonin is only low to moderate quality, and studies involved were small, averaging around 50 patients for chronic pain trials and 83 for surgical ones.
Still, melatonin has things going for it. It’s cheap, and it doesn’t carry the addiction risk that comes with opioids. Among trials that tracked side effects, the ones that turned up, mild nausea, dizziness, headaches, or drowsiness, tended to fade quickly. Taking it longer seemed to help more in chronic cases, though that comes from just a handful of studies. Nobody found a sweet spot for dosage; higher doses didn’t clearly beat lower ones.
Small Study Sizes Leave Big Questions UnansweredThis research has real gaps. Most studies involved were small, and almost none followed patients past three months, so nobody really knows if the benefits last. Researchers also couldn’t tell whether people with existing sleep trouble responded better to melatonin than those without, since none of the studies broke that down.
Next, the study’s authors want to see bigger trials that stick to a standard dose, run longer, and directly compare melatonin against tested painkillers. Until then, they see melatonin as something to pair with other treatments, not to replace them.
Muscle and joint pain affected up to 47% of people worldwide in 2020. A health problem this common makes even a modest, inexpensive option worth paying attention to. The evidence remains early and short-term, but it looks promising for chronic pain, even if the case for using melatonin after surgery is still thin.
Disclaimer: This article is for general informational purposes only and is not a substitute for medical advice. Anyone considering melatonin for chronic pain should talk with a doctor first, especially if pregnant, nursing, taking other medications, or managing a sleep or neurological condition.
Paper Notes LimitationsThe authors identified several important limitations. Most of the trials included in the analysis had small sample sizes, averaging around 50 participants per study in the chronic pain group and 83 in the surgical pain group. Nearly all studies provided only short-term follow-up data, with just one trial reporting outcomes beyond three months, leaving the long-term effects of melatonin on pain unknown. The researchers were also unable to determine whether patients who had pre-existing sleep problems responded differently to melatonin, because no included study analyzed that comparison directly. Subgroup analysis by specific pain condition or pain duration was not feasible given the limited number of studies in each category. Additionally, when multiple melatonin dose groups were reported in a single trial, data were drawn from the highest-dose arm only, which the authors acknowledge may have introduced some bias into the estimates. The overall certainty of evidence was rated as low to moderate using established evidence-quality guidelines.
Funding and DisclosuresAccording to the paper, one author is supported by a National Health and Medical Research Council Investigator Grant (Grant No. 1172928). Another author reported receiving personal funding from Eli Lilly, Eisai, and SomnoMed. A third author is supported by research funding from the National Health and Medical Research Council of Australia and by grants from national and international research foundations, including the Ramsay Research Foundation, Arthritis Australia, the NIHR, and the NIH, with all funds paid to her institution. In the context of these disclosed funding sources, the authors declared no conflicts of interest. The authors noted that ChatGPT was used during manuscript preparation for grammar checks and language refinements, with all research content, analyses, and conclusions developed by the authors themselves.
Publication DetailsAuthors: Kangchao Wu, Ting Him Ho, Paula R. Beckenkamp, Michelle Hall, Hanzhi Zhang, James Puterflam, Karin Due Bruun, Jianhua Lin, Christopher Gordon, Ron Grunstein, Manuela L. Ferreira, Paulo Ferreira | Journal: PAIN (published on behalf of the International Association for the Study of Pain by Wolters Kluwer Health, Inc.) | Paper Title: “Efficacy and effectiveness of melatonin for the management of musculoskeletal pain: a systematic review and meta-analysis of placebo and active controlled trials” | DOI: 10.1097/j.pain.0000000000004045 | Article History: Received 12 December 2025; Received in revised form 4 May 2026; Accepted 7 May 2026; Available online 30 June 2026 | PROSPERO Registration: CRD42023495805